- Warm welcome and thanks to our PEM team for joining: Dr. Rhodes and Dr. Weber!!
- Next week conference will be zoom, will go over some of the EMRAP cardio symposium
Dr. Kindschuh Oral updates
- STROKE CODE
- Will be switching from alteplase to tenecteplase (TNKase)
- 🔈 Goal to give thrombolytics <30 minutes
- Working on developing a script for TNKase consent.
- How we will get to <30 minutes TNKase administration:
- Stroke stretcher in triage
- Door to CT 10 minutes
- Standardized informed consent
- IVP TNKase as while in CT
- Dose: 0.25mg/kg (max dose 25mg) IV bolus over 10seconds.
- NOT compatible with dextrose solutions
- 🔈 How to order in epic? Type in TNKase (!!! DO NOT USE TPA !!!)
- Thrombectomy goal DoorInDoorOut: 120 minutes
- July median 135 mins
- September Inaugural quarterly stroke interventional conference
- Working on partnering with neurointervention for education
- GI Code
- 888 will respond after 4pm and on weekends
- Hand off to MICU is most important
- Make sure to reverse anticoagulation
- MTP
- Step wise process, per protocol: first delivery is 4 units pRBC, six other deliveries scheduled containing platelets, FFP 1:1:1
- Give 1:1:1 — PLT:FFP:RBC, not just pRBC
- Do NOT CHANGE the amount of units ordered in the MTP protocol, can always send unused products BACK.
- Attached PDF.
- Northwell blood cultures results you get in the middle of the night… What to do?
- Weekday, daytime → transfer to ED office
- Other times → email Dr. Kindschuh with MRN
- 7a: Resident Lectures: Raj – Pediatric Respiratory Illnesses / Mike Cyd – Pediatric Ortho / Denise – Anaphylaxis
- 830a: Robert – Tox Lecture – Marine Environmental Toxicology
- 9a: Dr Rizzo – Podcast Jam – Quick Hits #2:
- Organophosphate poisoning, metacarpal fractures, pediatric IV lines, abdominal stab wounds, and TXA for hemoptysis. PLEASE LISTEN BEFORE CONFERENCE***
- https://emergencymedicinecases.com/em-quick-hits-february-2019/
- 10a: Dr Cocchiara – Approach to ED Trauma
- 11a: Dr Gladstein – Intubation Cases + SIM
Raj – Pediatric Respiratory Illnesses

- Low SBP for kids (1-10yo) shortcut= 70+(2xage)
- DDx: bronchiolitis, PNA, whooping cough, croup
- Bronchiolitis
- Usually in winter months
- Age 0-2 year old
- H&P vs ABC? ABC
- Airway: Nasal suction w/ saline instillation
- Breathing: Warm humidified HFNC vs CPAP (o2 >90%)
- Circulation
- Consider in ill kids: albuterol, nebulized epi, steroids
- Children with fever and tachypnea make sure you give antipyretics, fever can cause children to be tachypnic (Dr. Rhodes, PEM attending)
- Intubation
- Tube size
- (Age/4) + 4 [uncuffed]
- Uncuffed: Only in neonatal period (Dr. Weber, PEM attending)
- (Age/4) + 3.5 [cuffed] ….. (Cuffed > 3 mo)
- (Age/4) + 4 [uncuffed]
- Use Miller blade
- Insertion depth = 3 x ETT size
- Tube size
- RSI/pretreatment meds
- Atropine
- 20-30 min before tubing== If <1yo to decrease secretions
- Ketamine
- Bronchodilator
- Atropine
- RSV is associated with apnea in children <6 months of age (Dr. Weber, PEM attending)
- Bronchiolitis – Who Needs to Stay (PEM Morsels)
- Toxic appearance (pale, lethargic), poor feeding, dehydration
- Respiratory distress
- <12 weeks and/or premature <34 weeks
- Pre-existing heart, lung or neurological condition
- immunodeficiency
- ☀️☀️🏝🏖Coney specifics☀️☀️🏖⛱
- URI test panel swab is the SAME as COVID
- Peds currently being transported out with respiratory support
- “At Coney, if you place HFNC you will need to convert to CPAP because EMS can only transport via CPAP.” (Dr. Rhodes, PEM attending)
- HFNC is titratable based on the weight of the child, CPAP you know exactly how much they are getting.
Denise – Anaphylaxis
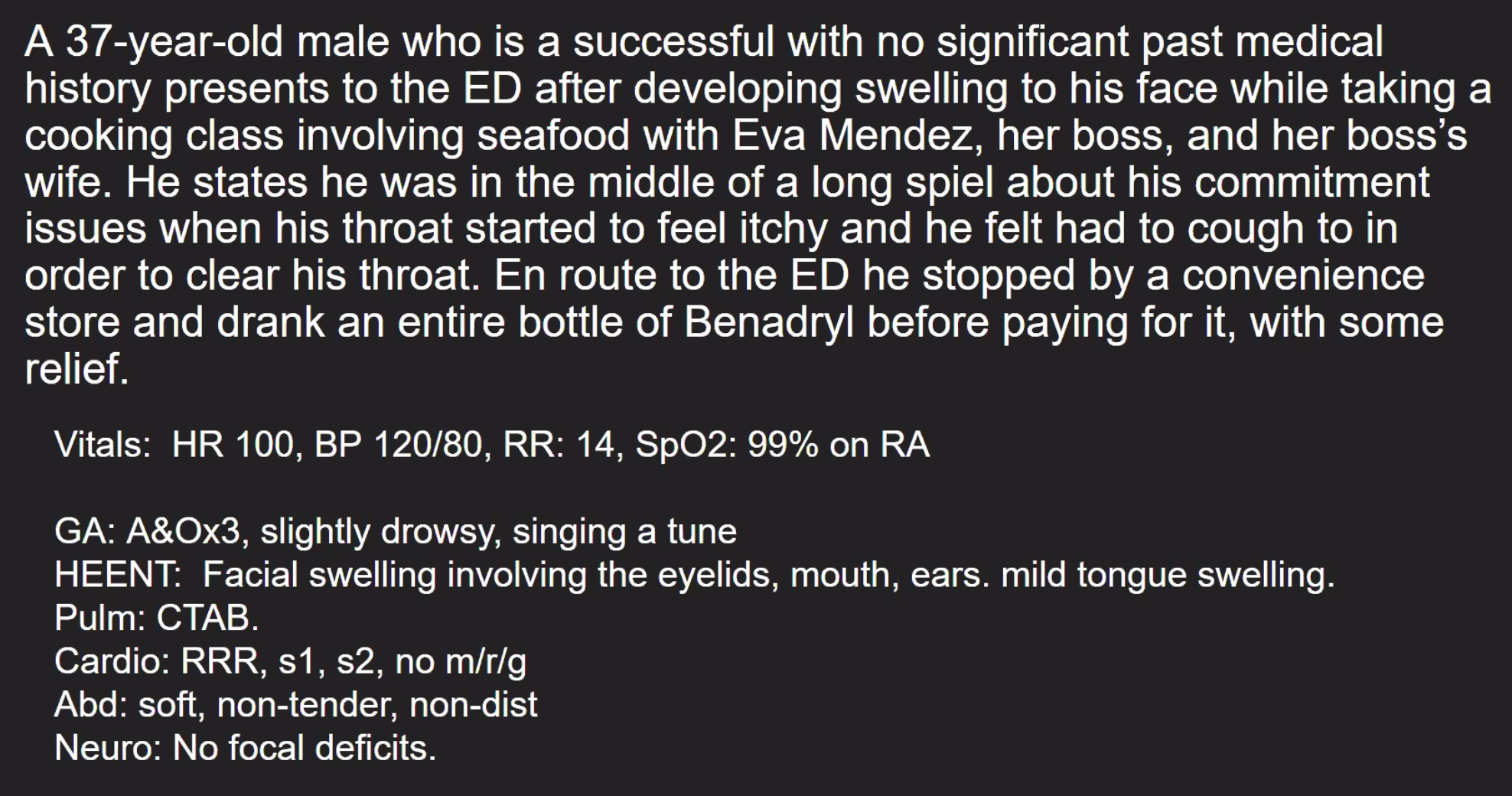
- Anaphylaxis criteria
- Skin symptoms + respiratory/GI/Hypotension/End organ damage
- 20% of anaphylaxis has no skin symptoms
- Symptomatic manifestations
- 90% cutaneous: hives, pruritus, angioedema, conjunctiva erythema and tearing
- 20% mucocutaneous = underdiagnosed
- 60-70% respiratory
- 30-50% GI
- 40-50% cardiovascular symptoms
- <15% neuro symptoms
- Precipitants
- Food (most common)
- Medications
- Insect stings
- Latex
- Aerobic exercise
- Idiopathic (rare)
- Anaphylaxis– EMCRIT
- Photos
- DDx: scombroid, atopic dermatitis, angioedema, transfusion reactions, contrast induced ‘reaction’, carcinoid syndrome, asthma
- Treatment
- Epinephrine IM 0.5mg (1:1000) to the lateral thigh q5/min x 3
- Epinephrine drip (or dirty epi: 1mg code cart epi into 1L NS)
- IVF
- Intubation? Fiberoptic, call anesthesia, cric ready
- On beta-blocker? Glucagon (careful can cause vomiting and airway obstruction)
- Adjunctive
- Diphenhydramine 25-50mg IVF
- Famotidine 20mg IVF
- Methylprednisolone 125mg IV
- Theoretical
- Methylene blue
- ECMO
- FFP
- MONOPHASIC vs BIPHASIC reactions
- Biphasic reaction occurs 10-20% of patients
- Biphasic reaction is more likely in a severe reaction
- Most biphasic reactions occur within 4 hours
- Observe for 4 hours prior to discharge
- Dr. Rizzo: ‘Steroid administration is dogma, no good evidence. Use epi and remove allergen.’


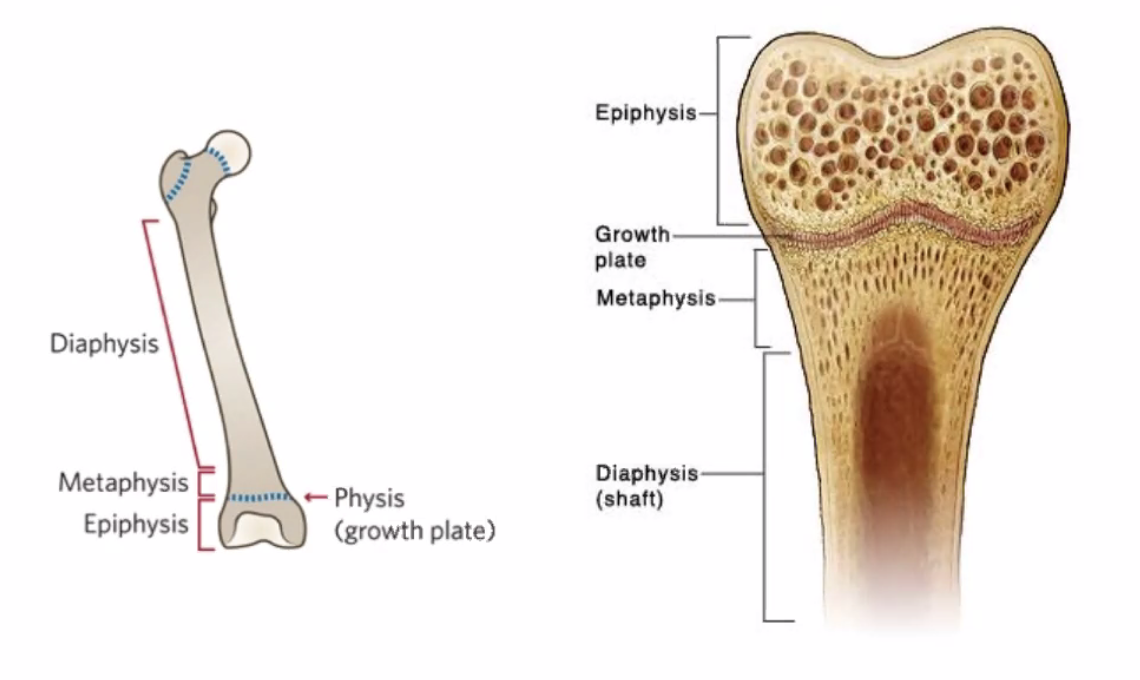
Mike Cyd – Pediatric Ortho
- Pediatrics Specialty Dashboard—High Yield peds orthobullets
- Bone anatomy review
- Growth plate = the physis
- Buckle = Torus fracture
- Greenstick
- Pathologic fractures: metabolic diseases, oncological causes, etc.
- Stress fracture = absent on initial xray, may see healing on repeat xray 2 weeks later
- Child abuse
- Long bone fracture in non-ambulatory child
- Metaphyseal corner fracture
- Rib, sternum, scapula, spinous process
- Multiple fracture in different stages of healing
- Always ask MECHANISM of Injury: ask multiple times for concern of abuse.
- Consider peds age for ambulatory considerations: rolling over, walking, standing up
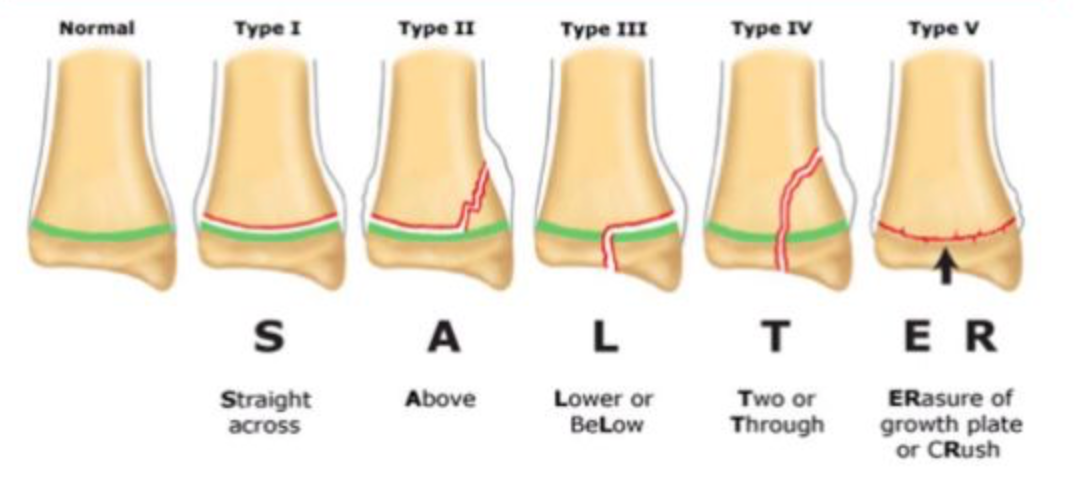
- Salter-Harris Classification
- Salter Harris Fractures – StatPearls – NCBI Bookshelf
- Type 1 = “Straight across”
- Soft tissue swelling, not always seen on Xray
- NON-OP: splint, ortho follow up outpt
- Ex: SCFE
- Type 2 = “Above” (most common)
- NON-OP: splint, ortho follow up outpt
- “Corner sign” = Thurston Holland fragment
- Type 3 = “Low”
- Ortho consult for Type 3-5
- Type 4 = “Through”
- Type 5 = “CRush/Rammed”
- Salter Harris Management
- Type 1 + 2 = splint and ortho follow outpatient
- Type 3 + 4 + 5 = ortho consult
- General treatment
- Pain control
- Open fracture: Antibiotics, ortho consult
- Neurovascular exam
- Consider compartment syndrome
- Dr. Rizzo: ‘Push for early ambulation in Salter 1 and 2, faster return to function’




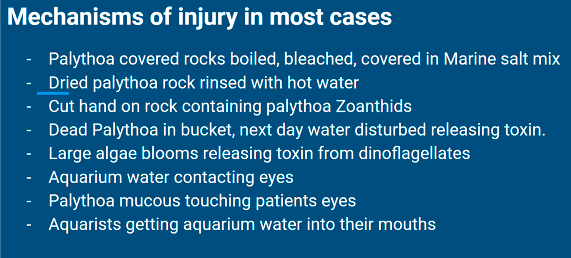
Robert – Tox Lecture – Marine Environmental Toxicology
- Aquarist = a person who keeps an aquarium
- Palytoxin: from Zoanthid corals, related to jellyfish, LD50 0.15-0.3 mcg/kg (super deadly)
- Binds to Na/K ATPase
- Causes: hemolysis of rbcs, violent contractions of heart and other muscle cells
- Heat-stable
- SYMPTOMS:
- Fevers, chills
- cough/hemoptysis, SOB
- Nausea
- Muscle pain
- Bitter metallic taste
- Burning in eyes
- Numbness
- Cardiac probs
- Depression
- High BP
- coma/death
- Tx: Supportive care
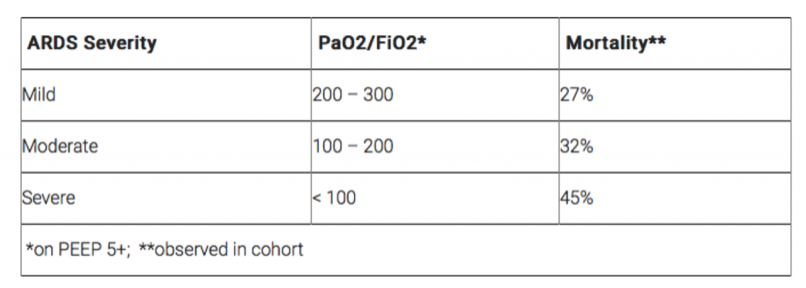
- ARDS severity classification
- Fishy Board Questions Review
- Ciguatera poisoning = cold–hot reversal
- Related to LARGE FISH
- Can be passed along in breast milk.
- Tx: supportive care
- Scombroid poisoning = Peppery flavor
- Histamine related
- Tx: antihistamine, supportive
- Sx within 10-30 mins
- Brevitoxin poisoning = shellfish poisoning
- VERY similar to Ciguatera –both have hot-cold reversal
- differentiated by food type
- VERY similar to Ciguatera –both have hot-cold reversal
- Tetrodotoxin poisoning = Parestesias
- Fugu pufferfish
- Ciguatera poisoning = cold–hot reversal
- Rob’s environmental plea ❤
- Beyond Sushi: Vegan Restaurant NYC – Vegan Sushi & More Manhattan





Dr Rizzo – Podcast Jam – Quick Hits #2: (LINK: EM Quick Hits 2 Organophosphate Poisoning, TXA for Hemoptysis, Metacarpal Fracture Rotation, Abdominal Stab Wounds, Pediatric IV Cannulation)
- Organophosphate Poisoning
- Cholinergic symptoms mnemonic
- Three B’s: Bronchorrhea, Bradycardia, Bronchoconstriction + Seizures (per Rizzo)
- Treatment
- Atropine
- MOA: directly antagonizes Ach
- Dries secretions: Give until chest is clear and pt is hemodynamically stable.
- Dose titration: 1-2mg/dose to start q5min
- Keep doubling dose until secretions are dry
- Pralidoxime (2PAM)
- MOA: Restores AchE
- Atropine
- Cholinergic symptoms mnemonic
- TXA for Hemoptysis (post-tonsillectomy)
- CRASH2 = mortality benefit in trauma within 3 hours
- CRASH-2 trial (NNT ~ 65 when given < 3 hours after injury)
- CRASH3= extrapolated CRASH2 to include TBI
- WOMEN Trial= TXA for postpartum hemorrhage
- 0.5% mortality reduction when TXA was given < 3 hours after onset of post-postpartum hemorrhage
- TXA for upper GI bleed? No evidence right now
- TXA for epistaxis? No evidence right now
- Post-tonsillectomy bleed
- Post-tonsillectomy hemorrhage
- Direct pressure if first approach
- Nebulized TXA
- Have all AIRWAY stuff read to go
- CRASH2 = mortality benefit in trauma within 3 hours
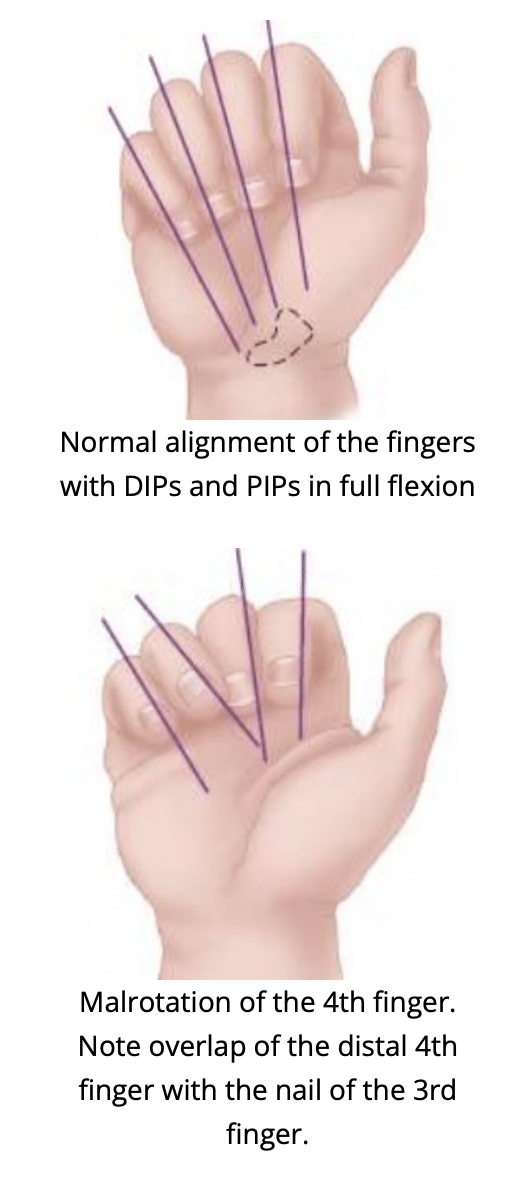
- Metacarpal Fracture Rotation
- Malrotation – bend fingers toward scaphoid, clinical dx, can miss on XR
- Abdominal Stab Wounds
- OR Indications
- Hemodynamic instability
- Bowel evisceration
- Peritonitis
- Impalement of the weapon/object
- CT can miss 10-20% on abdominal injuries, will need observation and serial abdominal exams
- Check for anterior rectus muscle violation
- US FAST exams are great, cannot rule OUT a serious pathology
- About 90% sensitive
- About 80-95% specific
- Get CT chest to r/o diaphragm injury
- OR Indications
- Pediatric IV Cannulation
- Consider EMLA
- Determine urgency
- US: better in older kids than younger kids-be careful with the pressure you’re using to not collapse veins.
- Secure IV!!! Use a board, tape, etc.


Dr Cocchiara – Approach to ED Trauma
- Next time
Dr Gladstein – Intubation Cases + SIM
- Oral boards case
- 28F found down on the stairs
- Moving uncontrollably in bed
- Initial steps in boards case:
- “What do I see when I walk into the room?”
- ABC
- Monitor, O2, IV, Saturation, BG, upreg
- Primary survey (ABCDE), undress patient, fully examine patient
- Need to place a c-collar! (consider trauma)
- You have 15-30sec to intubate, if unable, bag and restart
- 28F found down on the stairs
- Intubation preparation
- Suction
- Oxygen (NC + NRB)
- RSI meds
- Video vs Miller vs Mac
- Intubation indications (5)
- Oxygenation
- Ventilation
- Protecting airway
- Need for future procedure
- Control of agitated patient
- Confirm intubation
- End Tidal CO2
- Auscultate for bilateral breath sounds
- Chest XR (2-3 cm above carina)
- PLACE OGT AFTER INTUBATION–needs to be beneath diaphragm on CXR (~50-60cm)
- RSI meds
- Nasal intubation considerations: Nasal intubation: A comprehensive review




