Case Report (Sickle Cell Disease and Rhabdomyolysis vs. Renal Papillary Necrosis)
31 yo M w/ hx of sickle cell disease (SCD) presents to the ED c/o gross hematuria x 12 days. Pt reports hematuria began shortly after exercising and has remained constant with each episode of urination. Pt denies experiencing any similar sx’s previously. No abdominal pain, dysuria, back pain, fever, nausea, vomiting, fatigue, myalgias. Otherwise, pt states he feels perfectly normal. Pt was sent to ED from clinic for further evaluation.
Vitals stable. Physical exam unremarkable except for gross hematuria, visible in urine cup. Labs: Hgb WNL, CK 12,000, UA shows large hematuria w/ RBCs TNTC
Primary Differential: Rhabdomyolysis
Most likely Cause in this case: Exercise + Sickle cell
General Clinical Features: Myalgias, stiffness (MSK sx’s present about 50% of the time), weakness, fever, dark urine (This patient had red/dark urine, no other sx’s) Work -up: EKG, Total CK, UA, CBC, CMP, Uric Acid, LFTs, VBG, coags
Evaluation: CK typically 5x or greater increase above upper limit of normal). UA positive for blood but no RBCs, can see elevated CK w/o myoglobinuria, AKI might be present, electrolyte abnormalities may be present.
In this case, pt’s CK was 12,000 on repeat in ED and UA showed + blood with RBC’s TNTC 🡪 consider alternative diagnosis like renal papillary necrosis (RPN)
Background: RPN is associated with sickle cell hemoglobinopathies in addition to a variety of other causes. It is caused by the intravascular stasis and thrombosis caused by the sickling of RBCs which is precipitated by hyperosmolarity and low O2 within the renal medulla. This condition typically presents between 30-40 years of age. Painless hematuria is a common symptom seen in cases associated with SCD.
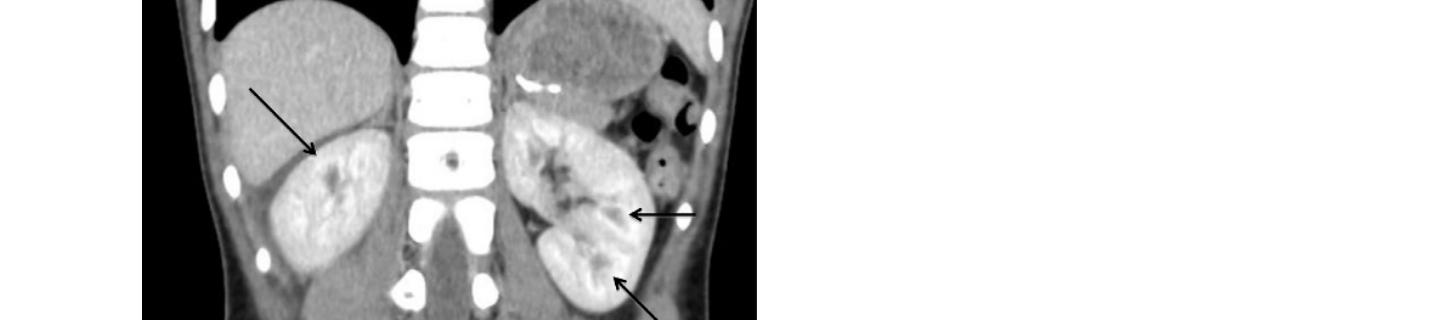
Evaluation: CT Abd/Pel is the gold standard in adults

Treatment: Hydration, alkalinization of the urine, broad spectrum antibiotics
Brief Discussion: The CK level and the UA was inconsistent for a classic case of rhabdomyolysis, therefore further work-up was indicated. To further evaluate painless hematuria for a condition such as RPN, cancer, or other etiology, a CT Abd/Pel and a urology consult should be heavily considered. Keep differentials broad. In this case most likely a combined case of rhabdomyolysis with another condition. Further work-up pending.
References:
https://wikem.org/wiki/Rhabdomyolysis
Henderickx, Michaël M.E.L., et al. “Renal Papillary Necrosis in Patients with Sickle Cell Disease: How to Recognize This ‘Forgotten’ Diagnosis.” Journal of Pediatric Urology, vol. 13, no. 3, 2017, pp. 250–256., doi:10.1016/j.jpurol.2017.01.020.
