Hey so after some reading just thought I’d share some info on ARVD. This can be tricky to diagnose for many reasons.
1) What does it stand for?
Arrhythmogenic Right Ventricular Dysplasia (common to replace Dysplasia with Cardiomyopathy). It’s the second most common death in young people <35yo with males more common than females (up to 20% of SCD in young).
(Bonus points: what’s the most common death in young people?) Interns..? ![]()
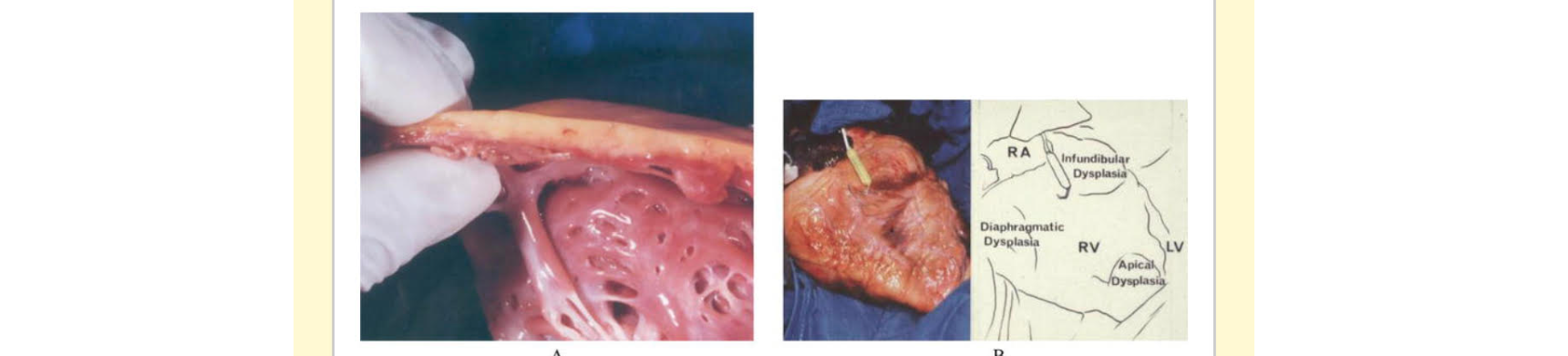
2) Two types: autosomal dominant (most common we see) and autosomal recessive (Naxos Disease, watch out for people with Italian or Greek decent) and there’s a fibro fatty replacement in the RV myocardium. It produces this classic “epsilon wave” which occurs at the end of the QRS complex. The reason for this occurrence is because you get postexcitation of the myocytes in the RV.
Essentially, some myocytes are replaced by fat which produces sort of an island of viable myocytes in a sea of fat ![]() . There then is a delay in excitation of those viable myocytes which causes this sort of “blip” or epsilon wave.
. There then is a delay in excitation of those viable myocytes which causes this sort of “blip” or epsilon wave.
These are Best seen in leads V1-4
The kicker is that it is only present in 30% of patients. So just because you don’t see them does not mean you cans exclude this deadly diagnosis.
Below are examples of what they might look like.

3) What are other EKG findings we can rely on?
-QRS widening >110ms in V1-V3
-Prolonged S wave upstroke in V-V3 (occurs in 95% of patients)
-TWI in V1-V3 (85% in patients)
-paroxysmal VTAC with LBBB
-evidence of RV failure /strain

4) Who should you be worried about that might have this?
– otherwise young healthy individuals (males > females 3:1) that present with syncope, palpitations or were in VF or VT or cardiac arrest
– family hx of SCD <45years old
– Greek or Italian decent
5) How do they present in my ED?
-27% will present with palpitations
-26% will present with syncope
-23% will present with VT/VF or cardiac arrest
– the rest are usually asymptomatic
6) What do I do now?
– PADs!!! Get ready and be prepared for crash/airway cart
– manage the VT/VF accordingly (shock, amio etc)
-Bedside ECHO may show RV dilation with hypokinesis
-STAT Cardiology consult
If they’re stable and asymptomatic, and you don’t see any epsilon waves, you can manipulate the ecg leads to better amplify the waves if you’re still suspicious.
These are called Fontaine Leads
The purpose of Fontaine leads is to magnify the atrial potentials and to be used to record epsilon waves. Literature says these types of leads are highly sensitive. A standard regular 12 lead ECG identified epsilon waves in 23% of patients. Those same pool of patients when using Fontaine leads identified epsilon waves in 75% (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2929850/)
You take RA lead and place on manubrium
LA lead over xiphoid process
LL lead and replace with V4


7) Disposition Time
– symptomatic—> CCU
-asymptomatic or incidental finding —> outpatient cardio follow up
They will need a Cardiac MRI +\- biopsy and ultimately ICD placement


Sources:
1) ARVD Wikem
2) ARVD LITFL
3)https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2929850/
