
Controlling the Upper GI Bleed…DROP THE TUBE!
The Case: 40-something yr old female, known alcoholic with history of esophageal varices presents to the ED with upper GI bleed. Pt is unstable and you gain control of the airway, place a left femoral cordis and start MTP with the rapid infuser. While
GI, Surgery, ICU are all at bedside debating what to do, you make numerous suggestions to place a Blakemore (or in our beloved Coney ED a Minnesota) with everyone looking at you in bewilderment on how to place one.
Indications to place the tube:
-The unstable patient that will not make it in time for endoscopy -Pt that had failed endoscopy management
-Temporary before TIPS procedure
Contraindications:
-known to have esophageal strictures -recent esophageal/gastric surgery
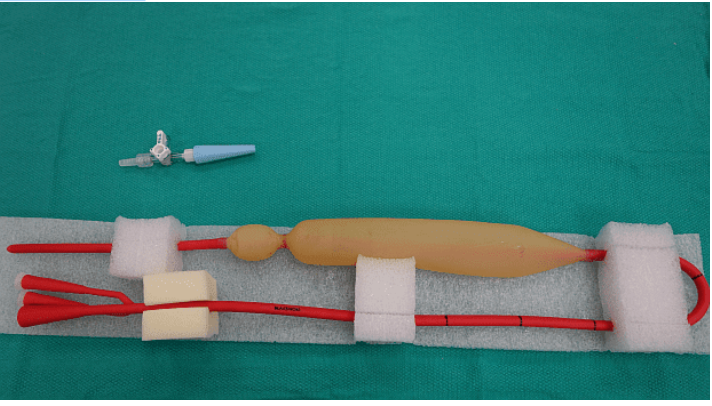
The Tubes: Minnesota
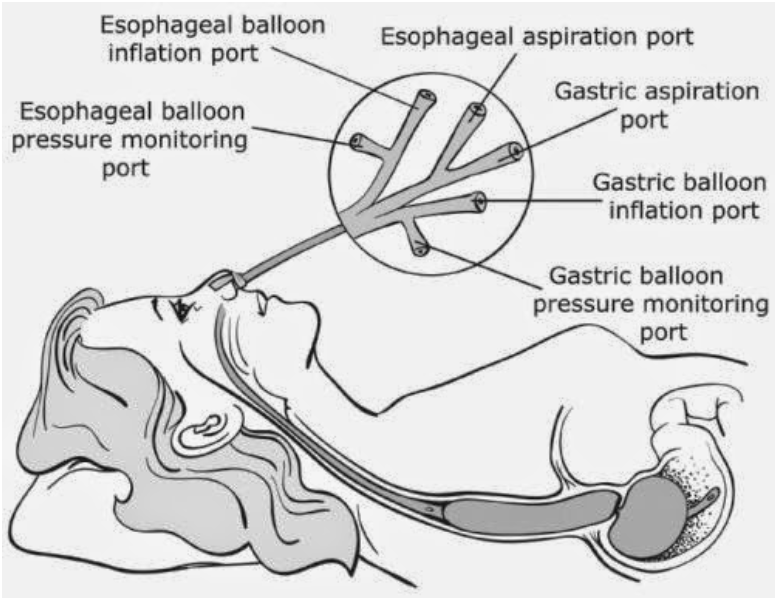
Blakemore
Important Differences to remember btwn tubes:
-Blakemore requires 250cc for the gastric balloon where Minnesota requires 500cc for the gastric balloon
-Blakemore has drainage for the gastric portion only, where Minnesota provides drainage for both the gastric and esophageal portions
-Minnesota has extra pressure monitoring ports (essentially useless) be sure to keep them closed
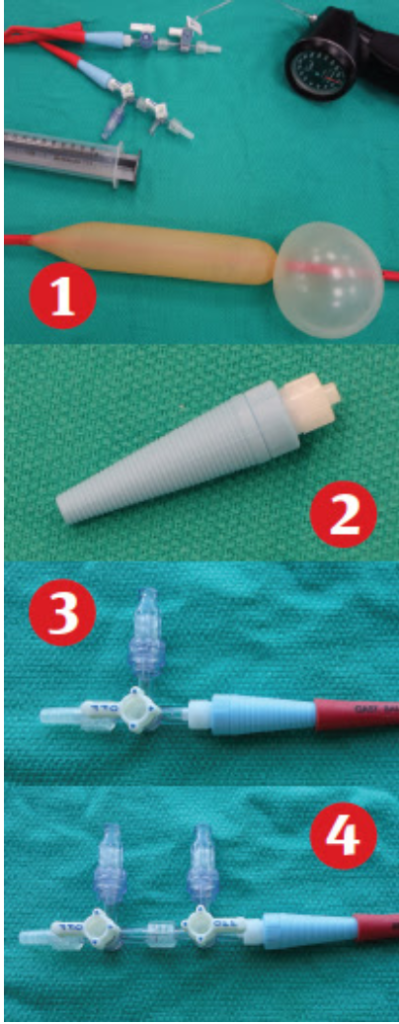
Preparing for the Procedure: be sure to have the following at bedside when prepping for tube placement
–> Blakemore/Minnesota Tube, NG tube (for marking), manometer (apparently respiratory should have one), 60mL syringe slip- tip syringe, 2 Christmas tree to luer-lok converters (unsure if this is in our ED), 3 three-way stop cocks, 3 med lock caps, Surgilube, Kling, 1 liter bag of fluid, IV pole, open container full of saline/water (for balloon check)
Placing the tube: **after securing the airway on your sedated patient**
1. Test balloons for air leaks in container of saline
2. Mark NG tube at the location 2cm above gastric balloon and then 2cm above esophageal balloon
3. Place Blakemore/Minnesota through mouth of the patient, stopping at the 50cm marker, test balloon placement with auscultation, add 50cc of air and obtain CXR to confirm gastric placement
4. With gastric placement confirmed add 200cc (250cc total) to the Blakemore and 450cc (500cc total) to the Minnesota gastric portions of the tube
5. Connect kling bandage to 1liter saline on one end and tube on the other draping the IV fluid bag over pole to create traction 6. Insert NG tube to part marked gastric meets the 50cm marker, suction both Blakemore/Minnesota lavage ports and NG tube
If bleeding still occurs it is time to inflate the Esophageal balloon
1. Pull back on the NG tube until the esophageal marker is at the 50cm marker, attach the manometer to the threeway stop cock placed on the esophageal port and inflate to 30mmHg
2. Suction to check for bleeding, if it continues inflate balloon to 45mmHg
For more clarification EM:Rap video on placement is pretty stellar:
Lessons Learned:
-Drop the tube and take control of the situation like we take control of an airway while all of our consults are around the bed debating what to do and the patient is continuing to decompensate


Have a good week everyone!
References:
- https://www.wikem.org/wiki/Balloon_tamponade_for_massive_GI_bleeding
- http://emcrit.org/emcrit/blakemore-tube-placement/ https://www.emrap.org/episode/placemenofa/placemenofa
- https://www.acepnow.com/article/place-blakemore-tube-ed-patient-upper-gi-bleeding-esophageal-varices/3/
