THE CASE: One of our not so regular alcoholic with pmhx of DM presented to the ED with eye pain with concerns for acute angle glaucoma. Upon discharge up to the eye clinic the patient states he was unable to walk. Muscle strength 5/5 and good reflexes.
What was going on here?? Was this man faking it to get an admission or was there something else going on??
WERNICKE’S ENCEPHALOPATHY vs WERNICKE-KORSAKOFF SYNDROME
Wernicke’s Encephalopathy
–Opthalmoplegia (nystagmus and lateral rectus palsy), ataxia, and disturbances of consciousness or mental activity (ALL 3 seen in <10% patients)
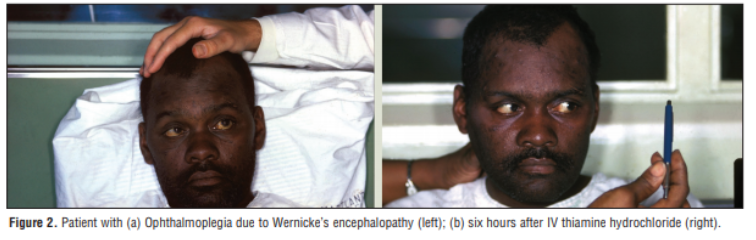
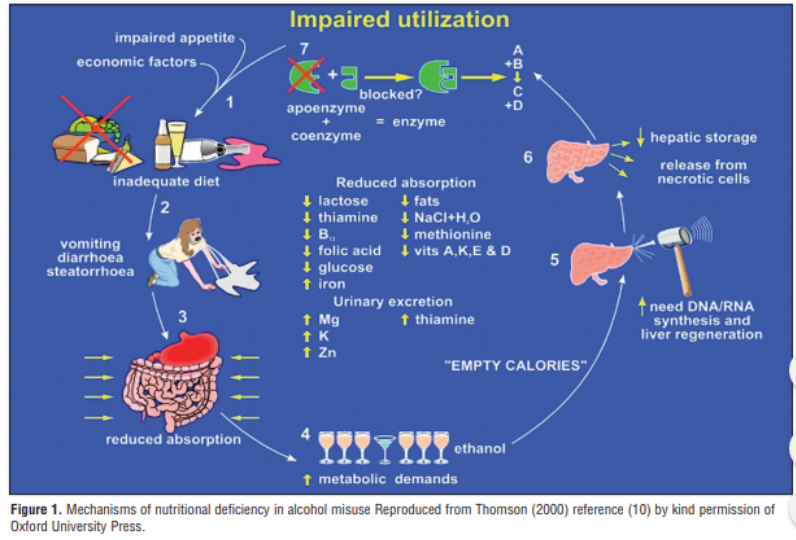
-Thiamine (B1) deficiency (Krebs cycle shuts down and ATP is depleted)
-Later progresses to IRREVERSIBLE Korsakoff’s syndrome if left untreated
Don’t just think it’s chronic alcoholics!
-happens in those with malnutrition or malabsorption (broaden the differential)
-bariatric surgery, AIDS, active malignancy, hyperemesis gravidarum (include hyperemesis cannabinoid syndrome too!), eating disorders, bone marrow transplant recipients and
our beloved CHF-ers on lasix
Other aspects of patient presentation
-hypotension or hypothermia
-elevated lactate
-lacking nutrition intake, oculomotor disturbances, any cerebellar dysfunction, AMS/memory impairment (>2 is
diagnositic of Wernicke’s Encephalopathy)
-also check pt’s magnesium level (hypomagnesemia is thiamine mimicker)
Prevention VS Treatment
-Prevention: send our alcoholics out on 100mg IV/IM or 250mg IM thiamine Can we just give them PO
–NOPE. An alcoholic’s absorption is crap. Our GI colleagues have found that no rmalization of their absorption does not occur for six-to-eight weeks of a high-protein, vitamin supplemented diet.
–DOSAGE: in our EM literature it is 100mg IV/IM (answer on the test) but what i have found by the GI people is 250mg IM for a minimum of 3-5 days is preventative (i’ve included the article below)
–Treatment: 500mg of Thiamine IV three times a day for 2-3 days (dilute in 50-100mL of NS and administer over 30min to reduce chance of anaphylaxis)
-This is followed by 250mg IV daily for 3-5 days
**REPLETE THE MAGNESIUM**
Wernicke-Korsakoff Syndrome (Korsakoff Psychosis)
–Why we should care? 10-20% mortality rate
-Develops as the Wernicke’s encephalopathy causes damage to the thalamus and hypothalamus **is irreversible disorder of ANTEROGRADE amnesia**
-Symptoms include:
~inability to form new memories ~severe loss of memory ~confabulation
~hallucinations
-Physical Exam: abnormal eye movement, decreased/abnormal reflexes, tachycardia, hypotension, hypothermia, muscle weakness/atrophy, coordination dysfunction
-see changes on MRI T2 images as the mammillary bodies light up like a Christmas tree
Only 25% recover, half improve but never completely recover, 25% show no response What about that whole “Thiamine before Glucose” thing??
-based on old-timey case report, least likely to send them into worsening encephalopathy
-Clinically: check the glucose, give the thiamine, give them a sandwich (order really doesn’t matter as long as they are administered), avoid prolonged glucose administration without giving thiamine
-what about my hypoglycemia unconscious alcoholic??
hypoglycemia hurts the brain A LOT MORE than thiamine deficiency, GIVE THE GLUCOSE
Think of Wernicke’s Encephalopathy as the “Acute” and Wernicke-Korsakoff as the “Chronic”

References:
- http://rebelem.com/wernicke-encephalopathy/
- https://www.uptodate.com/contents/wernicke-encephalopathy
- https://first10em.com/rapid-review-wernicke-korsakoff-syndrome/
- http://www.emdocs.net/thiamine-deficiency-pearls-pitfalls/
