Case: 5 yr old girl presents to the ED with toe pain. Mom states she saw that the toe was red and painful and looked like an ingrown toenail.
First, this mom is really bad at cutting toenails! after performing this procedure tell patients to not cut nails straight across as it is more likely to grow into the lateral nail fold, to stay away from tight shoes, and address rotated digits or toe deformities
Second, if you have a patient with this, start soaking the foot before you sit down to do the procedure, it will make your life
so much easier!
- Stage I –> erythema with slight edema and pain when you place pressure on the lateral fold
- Stage II –> stage I + signs of infection and purulent drainage
- Stage III –> stage I + stage II amplified with lateral nail fold hypertrophy
*in diabetic patients jump on this procedure, we know they are a little petri dish of foot infections
**in patients with vascular compromise, get podiatry or vascular on board for the removal (the only relative contraindication)
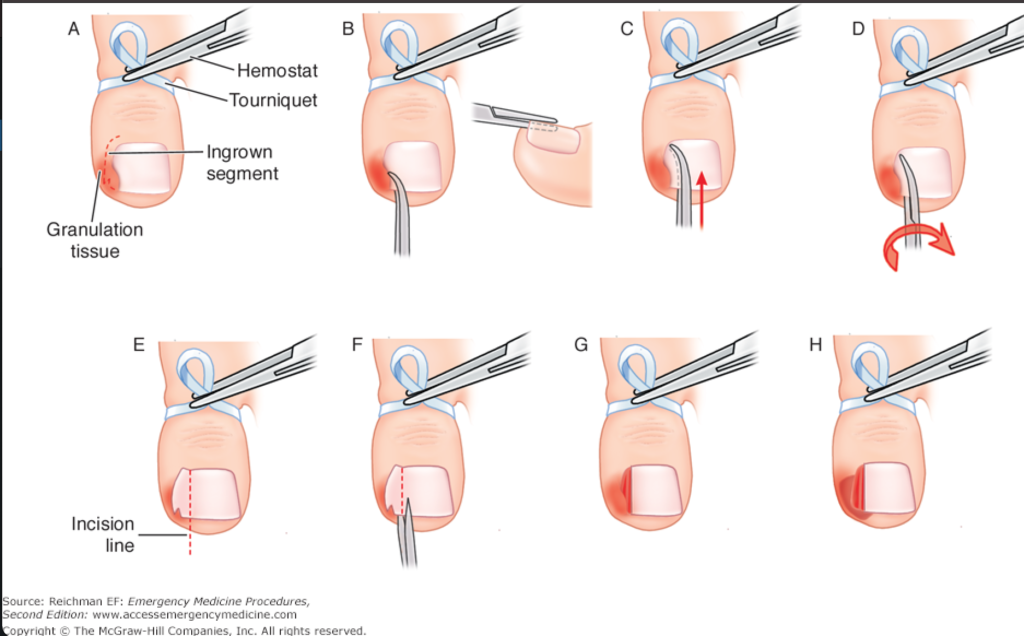
Start by anesthetizing the toe with either a digital block or direct infiltration
Next, cut the nail just medial to the ingrown nail
which can be done with a hemostat (depending on the thickness of the nail)
Then, lift the lateral aspect of the nail, gradually lifting the nail from the nail bed with a gentle upward motion
–> you can use silver nitrate to control any bleeding.
Lastly, cut out the spicule aspect of the ingrown nail, achieve hemostasis, and bandage the toe with oral abx if signs of infection.
Here is a diagram to follow along with: