- 7a: Mike Cyd – CCU/EKG lecture #2 / Mallory – Methadone Lecture
- 8a: Resident lectures: Ivan / Robert (please send me your topics soon)
- 9a: BREAK / Dr Jeong – Coney’s Complex Cases Review (Summer 2021)
- 1030a: Dr Kindschuh + Geoff – M+M Case – Posterior Stroke (Admin block lecture)
- 11a: Resident Meeting – Aug 2021 / Faculty Meeting Aug 2021
- GENERAL RESIDENCY UPDATES
- Link from Dr. Jeong: EMRAP Delta variant updates (8min podcast): LINK
- Dr Kindschuh – some housekeeping stuff about the Breezy Point Community Outreach event (next week)
- Replaces conference on Weds 08/11/2021
- Will have transport from CIH (time TBA) to Breezy Point prior to the start
- Dress Code: Business Casual
- Guys: Collared shirt (polo shirt OK), NOT jeans, NOT shorts, avoid tennis shoes if possible, NO TIE
- Girls: Probably whatever you want but who honestly knows (nice shirt, skirt/dress/pants, again no jeans)
- 30 Rosh Review questions will be assigned to all residents every week starting this week to help with inservice scores.
- 7a: Mike Cyd – CCU/EKG lecture #2
- Case 46M 2 hours of pressure like chest pain, exertional pmhx HTN, smoker, COPD, rhythm strip NSR
- ST depression V4-V6
- Repeat ECG within 10-15min
- Hyperacute T-waves, De Winter T-waves
- Hyperacute (Ischemia) vs Peaked (HyperK)
- Hyperacute = QRS can fit inside of the QRS (amal mattu)
- De Winter T-wave pattern
- STEMI equivalent: 2% of LAD occlusions
- More STEMI equivalents: LINK
- Next step:
- Meds: ASA 324mg (+plavix or Brilinta)
- Cath lab
- 100% LAD occlusion
- Peaked T wave differentials
- Prinzmetal angina (or MI)
- Hyperkalemia
- BER requirement (amal mattu)
- S-wave or J-wave in V2 or V3 — must be present
- De-Winter’s T waves (acute LAD occlusion)
- Get serial EKGs (usually not more frequently than q10 mins!)
- Dr. Steve Smith’s ECG Blog: Great reference for all things EKG & Emergency Department Cardiology
- OMI (Occlusion MI) & NOMI (Non-Occlusion MI) INSTEAD of STEMI/NSTEMI
- “STEMI criteria” missed ~30% of occlusion MIs
- Link from Dr. Jeong: OMI vs NOMI review




- Mallory – Methadone Lecture (addiction medicine lecture)
- 18yoM w hx of psych d/o, drug abuse and anxiety took Methadone + mirtazapine and was admitted for aggressive behavior/agitation to psych, then found dead 48hrs later.
- Naloxone:
- IN: 4mg
- IV
- 2mg if apneic
- 0.4mg IV if opioid-naive w minimal respiratory depression
- 0.05mg IV of opioid-dependent
- Observation period
- Heroin or other “typical” opiates (Oxy, Percocet, Norco, Heroin, etc)? Observe ~1-2 hours
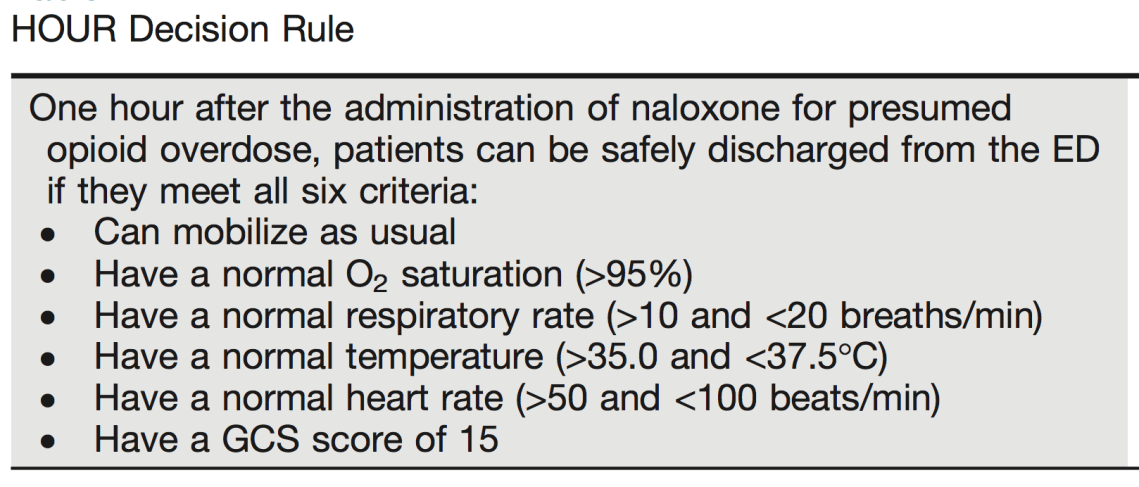
- HOUR Rule (when to discharge s/p narcan; NOT for Methadone OD)
- Methadone? 12-24 hours
- COWS score
- Heroin or other “typical” opiates (Oxy, Percocet, Norco, Heroin, etc)? Observe ~1-2 hours
- Methadone MOA: mu receptor agonist; Dosing: 10-20mg/day, increased in 10mg increments until withdrawals sx’s are controlled
- 20mg daily MAX allowed to be given in ED (unless they have their ID cards)
- If giving home dose, you MUST call the program & document the person who verified the dose… Otherwise, just give 20mg
- May need to half dose if pt has not taken methadone
- “A methadone dose of 10 mg intramuscularly or 20 mg orally significantly reduces the Clinical Opiate Withdrawal Scale score in ED patients with opioid withdrawal.” – Su M.K., Lopez J.H., Crossa A., et al. Low dose intramuscular methadone for acute mild to moderate opioid withdrawal syndrome. (Am J Emerg Med. 2018; 36: 1951-1956)
- QTC prolongation → Torsades 💩… Give ALL the Magnesium!
- Conservative definition of QTc prolongation: >470ms in men and >490ms in women
- Observe for 12-24 hours
- Buprenorphine (Suboxone) MOA: mu partial agonist + Narcan (pure antagonist)
- Use COWS score! 🐮



- Vivitrol (injectable naltrexone)
- MOA: Full opioid antagonist
- Will precipitate withdrawal symptoms if ANY opioids in system (No opiates at least 3-5 days, No Methadone for 7-14 days)


- “If you save one person, you save the universe.” -Dr. Radeos on Chinese proverbs.
- Imodium (Loperamide) – mu agonist but doesn’t cross BBB, still prolongs QTc
- 8a: Resident lectures: Ivan – Alcohol
- Alcoholics w trauma: low threshold to CT– ETOH causes brain shrinkage like old age, increased risk of bleeding.
- ADH becomes saturated at low concentrations
- CP 450-2Eq metabolism becomes more important at higher etoh concentrations or in chronic drinker
- ETOH metabolism: 30mg/dL/h in tolerant drinkers; non-tolerant 15-20 mg/dL/h
- Metabolic disorders
- Hypoglycemia
- ALWAYS GET A FS
- More common in peds 2/2 less glycogen storage
- HypoMag
- Dietary deficiency
- Malabsorption
- Incr urine excretion
- Ketosis
- Prolonged QT
- Vit D deficiency
- Tx: EKG, Monitor, Magnesium repletion
- HypoNa (Beer potomania)
- HypoNA Causes: beer potomania, pseudohyponatremia, SIADH, cardiomyopathy, cirrhosis, cerebral salt-wasting syndrome
- Presentation: Neuro- AMS, FNDs, seizures
- Dx: r/o other causes, BMP, beer drinking, low urine osm/low urine Na concentration
- Tx: Water restriction, SLOW repletion, if seizing then hypertonic saline vs crash-cart hypertonic NA-bicarb
- Alcoholic ketoacidosis (AKA)
- Diff with DKA
- AKA higher pH, lower potassium;
- BHB is primary anion in AKA
- Tx: IVF, dextrose, thiamine, Folic Acid, Mg/K (dependent)
- NOT insulin
- Diff with DKA
- Wernicke/Korsakoff
- Wernicke Triad: confusion, ophthalmoplegia, ataxia
- Korsakoff: IRREVERSIBLE amnesia, confabulation
- Tx: IV Thiamine 500mg TID for 2-3 days followed by 250 for 3-5 days
- Hypoglycemia
- Resident lectures: Robert – Alcohol Withdrawal
- Fine while drinking / drunk
- When EtOH goes away, CNS is PISSED
- Tongue fasciculations = UMN issue; we should call them tongue TREMORS
- SEIZURES: generalized tonic clonic
- Hallucinations — but patient knows they are NOT real
- Delirium tremens:
- onset after last drink: 48+ hrs
- AMS defines DTs
- No evidence of coma or other evolving neurocognitive disorder
- Autonomic instability
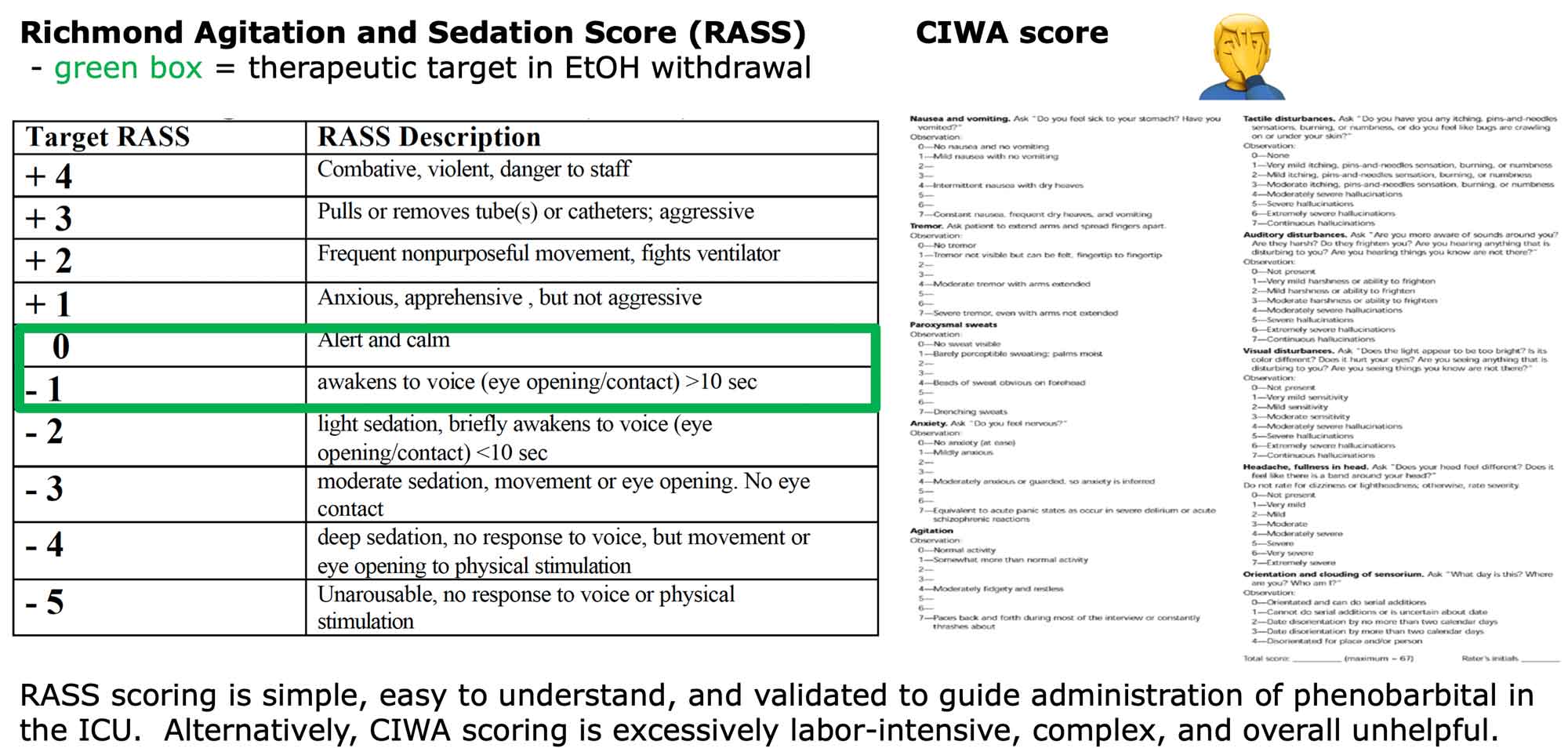
- CIWA score (serial-like a lab or vital sign)
- <8 maybe discharge
- >20 admit and may need MICU
- RASS score–used in patients who are NOT speaking
- Treatment
- Benzos
- Benzo equivalency chart
- Valium (Diazepam)
- IV pushes q5-10min
- 10mg x2 → 20mg x3 → 40mg x3 = 200mg TOTAL
- Ativan (Lorezapam) –can cross BBB, metabolized outside the liver
- Versed (Midazolam)
- Librium (chlordiazepoxide)
- IV BZDs for seizure – time to effect and duration:
- Phenobarbital
- Propofol – GABA agonist, for intubated patients generally
- Dexmedetomidine – alpha 2 agonist, s/e hypotension + bradycardia
- Does NOT treat etoh withdrawal, usually only adjunct therapy
- Fixes vitals but not the cause, NO GABA activity
- Ketamine – NMDA receptor antagonist, NMDA receptors are NOT downregulated in chronic EtOH, chronic BZD use, prolonged seizures;
- s/e: tachy, HTN, laryngospasm, secretions
- Thiamine –
- Water soluble
- Maximum body stores: , exist primarily in skeletal muscle, amount to ~30mg and can be depleted in as littel as 20 days in a patient inadequate intake, malabsorption or excess metabolic demand
- TACHYCARDIA is earliest symptom of thiamine deficiency, can develop as early as 9 days after intake ceases
- Give with the alcoholics (water soluble so it’s REALLY hard to overdose)
- Prophylaxis 100mg IV
- PO is unpredictable
- Thiamine deficiency → unexplained high lactate
- Benzos

- Dr Jeong – Coney’s Complex Cases Review (Summer 2021)
- CASE 1: 66 y/o hx of DM, HTN, smoking presenting w/ seizure vs syncope
- Seizure = aura, post-ictal, lateral tongue biting, few hours, high CK
- Syncope = flushed, hot/cold, 3-30 seconds, young age
- JournalFeed 10/20 Seizure vs Syncope Rule
- <10 jerks favor syncope
- >20 jerks favor seizure
- ST Elevation in aVR, Leads III, aVF; STD V4-V6, Lead I, aVL; T-Wave inversion vs biphasic in aVL
- Case continued:
- Sent emergently to Cath Lab (STEMI Code activated)
- Cath report: 2 vessel disease (RCA with complex calcified lesion 95% occlusion, mid-LAD with 80% lesion with patent flow)
- Due to complexity of RCA lesion and absence of overt culprit lesion, decision was made by Cardiology team to stage intervention, and pursue transfer to MMC vs BHC
- While awaiting transfer overnight, patient had multiple episodes of polymorphic VT (Torsades), Pacemaker called overhead, CPR performed, and defibrillated back to NSR
- Emergently transferred to MMC Interventional Cardiology extremely late at night ~0200
- From Dr. Jeong: Convulsive syncope research link: Convulsive Syncope Induced by Ventricular Arrhythmia Masquerading as Epileptic Seizures: Case Report and Literature Review
- Takeaway points:
- Use objective findings (EKG, pmhx) vs subjective findings (chest pain description)
- Worry about things that kill (MI more worrisome than new-onset seizure)
- When in doubt (or conflicting statements from consultants), do the thing that will protect the patient


- CASE 2: 600lb patient with respiratory failure
- 600lb person = still normal human size lungs
- The Crashing Obese Patient (PDF)
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6404698/pdf/wjem-20-323.pdf
- Reverse trendelenburg — can take weight off chest and give lungs room to expand
- Ramped position better than sniffing
- Reverse trendelenburg helpful
- Ear to sternal notch in same horizontal plane, face parallel to ceiling
- The CRASHING obese patient
- Links from Dr. Jeong:
- CASE 3: 23yo Stab Victim
- 23yo stabbed in L anterior chest
- ABCs stable, primary survey intact, EFAST neg
- Crazy story, no summary, you had to be there, sorry
← Jordan’s face
- If stabbing victim comes to hospital (especially walk in) lock hospital down, expect retaliation
- CASE 4: 54 y/o code 5, respiratory arrest
- Brought from hallway apnea and “running wheeled” to resus room
- 100% o2 sat but no chest wall rise, ventilatory problem, not oxygenation
- ABCs first
- Oxygenation vs ventilation
- You can’t NRB someone if their diaphragm isn’t moving
- CASE 5: 70yo with refractory septic shock
- Maxed on pressors (Levo, epi, vaso) and fluids, still hypotensive 50/30
- “Did you give steroids?”
- “Nobody dies in the ED without getting steroids”
- Give 100-200mg Hydrocortisone
- Links from Dr. Jeong:


- Dr Kindschuh + Geoff – M+M Case – Posterior Stroke (Admin block lecture)
- *** EM:RAP – C3 – Approach to Dizziness ***
- How to Not Miss Posterior Stroke — JournalFeed
- 49M with headache, nausea, vomiting
- FS 202, Istat K = 33, AG 22, LA 3.5
- Meclizine, pepcid, valium, no response, CT head negative, MRI ordered, neuro consulted
- PE: +horizontal nystagmus, +vomiting
- Neuro consult: no tPA because time of onset unclear
- MRI = cerebellar stroke
- Discharged home 2 days later, modified Rankin = 0
- Problem? CT was done after 1 hour, should have been done immediately, delayed diagnosis
- Gait testing is *super* important — best neuro test
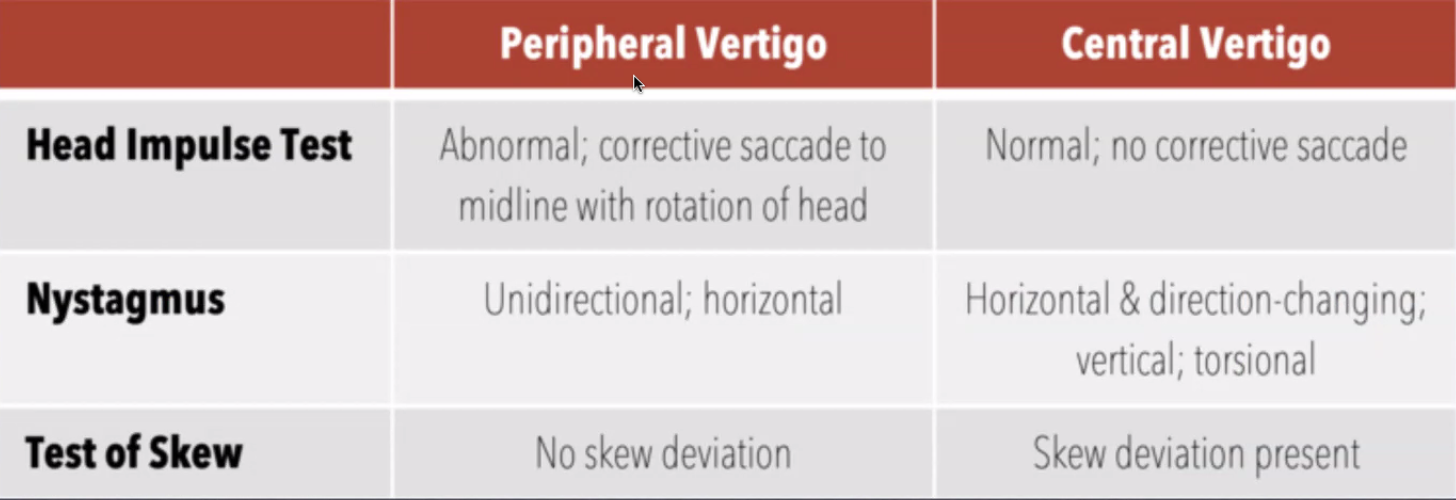
- HINTS exam
- tPA within 3-4.5 hours of onset and absence of contraindications
- Get a CT head non con but ALSO CTA head and neck for r/o LVO, MRI after if negative
- MRI missed 10-20% of posterior strokes — consider tPA


- 11a: Resident Meeting – Aug 2021




